
Research Article | DOI: https://doi.org/10.31579/2578-8868/199
Rehabilitation Medicine Service, Brigg, Uk
*Corresponding Author: Khin Maung Bo, Rehabilitation Medicine Service, Brigg, North Lincolnshire Uk,
Citation: Khin Maung Bo. (2021) Muliple Sclerosis, Corpus Callosum & Epilepsy. J. Neuroscience and Neurological Surgery. 9(3); DOI:10.31579/2578-8868/199
Copyright: © 2021 Khin Maung Bo, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 15 July 2021 | Accepted: 28 July 2021 | Published: 06 August 2021
Keywords: multiple sclerosis; epilepsy; corpus callosum; re-entrant circuit
There is a difference in prevalence of Epilepsy in General population & MS patients. Interical Epileptiform Discharges (IED) positivity in EEG is also different in the above two populations. Demyelination slows down the conduction speed of axons and author is proposing that different speed of conduction in adjacent axons can generate re-entrant circuits. If the reentrant circuits involve Corpus callosum (CC) fibers, seizure activities of MS can be triggered. DBS applied to CC can terminate the seizure attack of MS like Vagal Nerve Simulator (VNS) in terminating seizure in general population.
AV= Atrioventricular, CC= Corpus callosum, DBS= Deep Brain Stimulation, IED= Interictal Epileptiform Discharge, REC= Re-entrant circuit, SVT = Supraventricular tachycardia, VNS= Vagal Nerve Stimulator, VICS= Variation in conduction speed
Epilepsy in general population:
The prevalence of epilepsy in general population is 0.97% (Joint Epilepsy Council of the UK and Ireland 2011). Standard investigation for Epilepsy is EEG, looking for IEDs but only in about one third of epileptic patients showed IEDs on EEG.
Epilepsy in MS sufferers:
According to my experience, the prevalence of Epilepsy in Multiple Sclerosis population is around 4% and EEG in this population does not show IEDs.
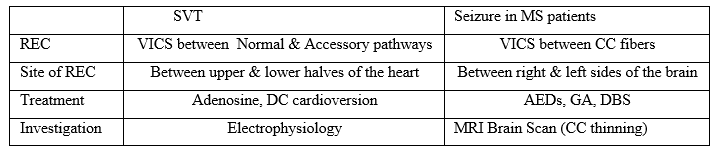
The comparison between the two populations is described in Table 1,

To propose a concept that can explain the difference in prevalence between general population and MS patients
In MS, it is the white matter axons that are affected by demyelination. As we all know, demyelination slows down the conduction speed in the axons. The speed of conduction in axons will vary depending on the extent of demyelination in the axons. This will result in variations in conduction speed (VICS). VICS can create Re-entrant circuits (REC). It is like in Atrio-ventricular re-entrant circuits of AV conduction bundle in the heart. The RECs in AV conduction bundle can trigger Paroxysmal SVTs and can even lead to Cardiac arrest.
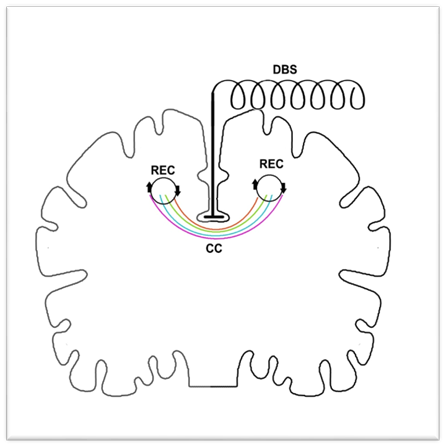
In the brain, the CC (containing millions of axons) connects the two sides of the brain and the conduction is in both directions. It is the most likely potential point where re-entrant circuits can occur if there is VICS in the axons (Figure 1).
The comparison between RECs in AV node and CC is mentioned in Table 2.
The other significant finding in my experience is that all of MS patients with epilepsy were found to have significant thinning of the CC on MRI brain images. Thinning of the CC is the evidence that the demyelination process involves CC fibers (Figure 2).
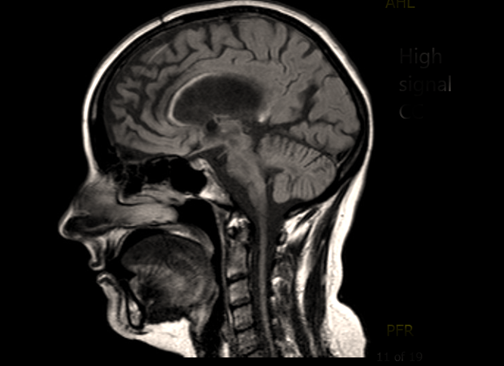
The scan showing significant thinning and high signal of Corpus Callosum in Multiple Sclerosis patient who started having seizures and EEG did not show Interictal Epileptiform discharges
If this hypothesis is proven, Deep Brain Stimulation (DBS) applies to CC (Figure 1) could be a new treatment in terminating seizures in MS sufferers (like applying Vagal Nerve Stimulator in Epilepsy in general population). DBS to CC is like a temporary electrical Corpus callosotomy.
Demyelination can create VICS in axons. If the VICS axons are adjacent to one another, RECs can be created. If RECs involves CC axons, seizure activity can result. This is my proposed pathophysiology for epilepsy in MS. DBS applying to CC can be a promising intervention in terminating seizure activity of MS sufferers.
Conflict of Interest
There is no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
